
November 29, 2022
Note: This resource is intended to be useful both as a standalone document, as well as the seventh part of Business Group on Health’s Value-Based Purchasing Guide. Click the link to access additional parts related to other elements of employer value-based purchasing strategy.
Employers have several plan design and engagement options for encouraging patients to seek care from providers in value-based arrangements. Generally, the more proactive an employer is about steering patients toward providers in value-based arrangements, the more likely they will benefit from improved care from those providers. Employers with highly engaged or incentivized employees will likely find provider partners more willing to contract with them; providers taking on financial risk for cost and quality want as much control as possible over the health care utilization of the patients they’re responsible for. Some of the engagement steps that employers can take include communications, cost sharing and other financial incentives and attribution.
Below are several ways employers can encourage employees to seek care from high- quality providers operating in value-based payment arrangements.
Communications
- Focus communications to employees on improved health outcomes, access to care, patient experience and the financial benefits of choosing a Center of Excellence (COE) provider, an accountable care organization (ACO) plan, direct primary care practice or other provider operating in a value-based arrangement.
- Consider utilizing messages coming directly from health care providers. For example, an ACO provider can “welcome” employees into a new high-performance network (HPN) or ACO at the beginning of a partnership, or a COE provider can reach out to employees with a recent diagnosis in their area of expertise about options within their benefits plan to get high- quality care at their facility.
- Health plans should reiterate this message during open enrollment, within their provider directories and other times throughout the year as appropriate.
- Where possible, invite providers who participate in value-based care partnerships to local employee health fairs to present on their practice and answer questions. Providers from systems with a great reputation in a given market or nationally can be particularly effective at engaging employees, though reputation should not be a deciding factor in who an employer or health plan contracts with in a value-based arrangement.
- Include providers in vendor summits to make direct connections between them and other third-party vendors you work with to encourage cross-referrals.
- Employers can encourage or require third-party vendors to cross-promote each other’s services, including value-based network plans like ACOs and COEs. Other services include concierge, transparency, employee assistance programs (EAPs) and other vendors an employer contracts with.
- Precision navigation to value-based providers should focus on employees who can most benefit from these types of arrangements, such as people without a regular source of primary care or those with a chronic condition that could benefit from an ongoing source of effective care.
Financial Incentives
Financial incentives for seeing providers in a value-based care arrangement or choosing a value-based health plan can be used in conjunction with other engagement strategies to help patients understand the value of and benefit from these arrangements.
Incentives to See Providers in Value- Based Arrangements Embedded in a Broader Preferred Provider Organization (PPO)
- 1 | Place providers participating in value-based arrangements in the preferred cost-sharing tier, or as the only providers in a preferred tier. For health savings account (HSA) compatible plans, members will need to hit their deductible prior to receiving these incentives. For this reason, account-based incentives listed below may be more effective.
- 2 | Offer health plan options with lower premiums tied to the network of providers participating in value-based arrangements. Exceptions should be made for issues like emergency care, mental health, specialized care and treatment outside a patient’s local market.
- 3 | Remove cost sharing entirely for patients seeing providers in capitated models like direct primary care
Examples of other financial incentives include:
- Contributions to HSAs or health reimbursement arrangements (HRAs) for actions like selecting a health plan wrapped around a high-value network, picking a primary care provider in the value-based network or completing their first well-being visit with a provider in the value-based network.
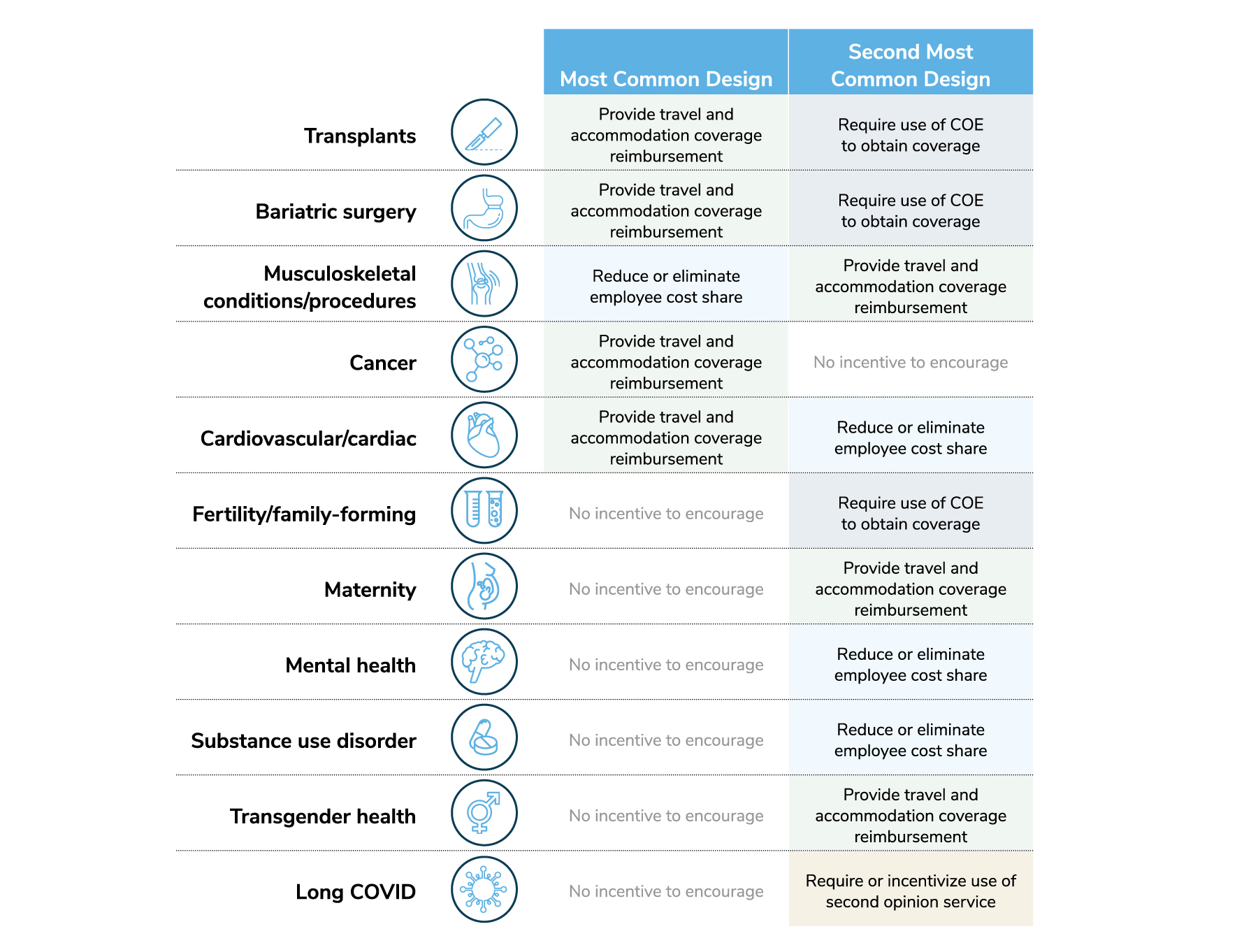
Source: 2023 Large Employers’ Health Care Strategy and Plan Design Survey
- Lower premiums for people who select a health plan tied to an HPN or ACO.
- Low to no copays for generic medications, virtual visits, primary care visits and high-value services delivered by a provider in a value-based arrangement.
- No cost share and free travel benefit for some COE services. There are a handful of case studies where employers have covered all costs associated with surgeries that are performed by select high-performing providers.
Attribution
How patients are assigned to providers can have a significant impact on a value-based plan’s ability to improve health and reduce costs. For providers in a value-based plan, knowing their list of assigned—or attributed patients—enables them to do outreach, promote prevention and proactively manage care. As part of contract negotiations, value-based plans may ask or even stipulate that partnering employers encourage, incentivize or require their employees to select a PCP or provider group to whom they will be attributed for the plan year.
Codifying the relationship between a patient and the physician who is responsible for the patient’s care, as well as for associated costs, is also necessary for determining the financial performance of the value-based plan and its participating providers.
There are two major strategies for facilitating patient attribution. Both have potential benefits as well as downsides, and employers should understand them when engaging with a value-based plan:
- 1 | “Passive attribution” based on prior year’s claims. Plan members are attributed to a PCP based on their previous claims history and which PCP they saw most in previous years. The automatic nature of this approach reduces plan member tasks at the beginning of the year and potential disruption associated with changing providers, but it may limit effectiveness of some of the engagement strategies described above. Some patients have little to no claims history and without a proactive step, there is no connection made between provider and attributed patient.
- 2 | “Active” PCP selection at health plan enrollment. Plan members select an in-network PCP participating in the value-based arrangement when enrolling in a health plan or when a new employer requirement for active selection is introduced. Here, there is a proactive element to the patient-provider pairing, which can be used to create awareness on the part of employees about the benefits of their PCP relationship. Provider groups often prefer active PCP selection, but it can be a cumbersome exercise for employees.
Attribution to a Provider Leads to Attribution to a Value-Based Care System
When a patient is attributed to a physician participating in a value-based care arrangement like an ACO or primary care practice, it is the broader system or practice the patient is attributed to that is held accountable for outcomes and cost of care for that patient (and the system’s entire attributed patient population.) Patient-physician attribution is important to encourage connections between a patient and their provider, but in effective team-based care, there will be an entire team or system around that PCP that will ultimately best care for that patient and be held accountable for contracted quality and cost targets.
In recognition that for some patients, their regular source of care is not a PCP, but a specialist (e.g., an OBGYN for a young woman or an endocrinologist for a patient with diabetes), some value-based care arrangements will allow for attribution to specialists participating in the value-based network. As above, the outcomes for these patients’ and the total cost of care will generally be the responsibility of the entire system, but avoids the situation where a patient is attributed to a PCP with whom they have no relationship while they separately get many of their care services from a specialist.
Conclusion
The effective rollout of value-based arrangements requires many actions enumerated in this section, such as clear personalized communications about the benefits of participation, some level of attribution and plan design features that encourage patients to select and seek care from participating providers.
Employer Recommendations
- 1 | Ask your health plans and consultants for comparisons of employee engagement/participation with value-based care (e.g., ACOs, HPNs, COEs, etc.) across their book of business; consider engagement strategies similar to those with the best results.
- 2 | Align the aggressiveness of your communication, financial incentive structure and attribution strategy with your level of confidence in your value-based care providers. Some employers are willing to completely waive cost-sharing for health care services delivered in some COEs or DPC practices because of the results they’ve achieved.19
- 3 | Where possible, include messaging from the providers who participate in value-based arrangements with your standard employee communications. Where an employee’s health plan selection is tied to a value-based contract (e.g., a directly-contracted ACO or HPN) communications directly from providers “welcoming” plan members to the plan can create trust and augment messaging. Some employers have also found success in joint communications when messaging around new value-based partnerships.
More Topics
Articles & Guides- 1 | Centers for Medicare & Medicaid Services. Performance Year 2021 APM Performance Pathway: CMS Web Interface Measure Benchmarks for ACOs. Quality Payment Program. Accessed October 11, 2022. https://qpp-cm-prod-content.s3.amazonaws.com/uploads/1306/Performance%20Year%202021%20APM%20Performance%20Pathway-CMS%20Web%20Interface%20Measure%20Benchmarks%20for%20ACOs.pdf
- 2 | The Leapfrog Group. Preventing and Responding to Patient Harm. Leapfrog Ratings. Accessed October 11, 2022. https://ratings.leapfroggroup.org/measure/hospital/preventing-and-responding-patient-harm
- 3 | Agency for Healthcare Research and Quality. About CAHPS. July 2022. Accessed October 11, 2022. https://www.ahrq.gov/cahps/about-cahps/index.html
- 4 | Conti R et al. Projections of US Prescription drug spending and key policy implications. JAMA Health Forum. 2021;2(1). https://jamanetwork.com/journals/jama-health-forum/fullarticle/2776040. Accessed November 8, 2022.
- 5 | Business Group on Health. Emerging Trends in Cancer Care. October 25, 2021. https://www.businessgrouphealth.org/resources/emerging-trends-in-cancer-care. Accessed November 8, 2022.
- 6 | Golden W et al. Changing how we pay for primary care. New England Journal of Medicine Catalyst. November 20, 2017. https://catalyst.nejm.org/doi/full/10.1056/CAT.17.0326. Accessed November 8, 2022.
- 7 | Bitton A et al. Off the hamster wheel? Qualitative evaluation of a payment-linked patient-centered medical home (PCMH) pilot. The Milbank Quarterly. 2012 Sep; 90(3): 484–515. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3479381/. Accessed November 8, 2022.
- 8 | Primary Care for Boeing’s Mesa Employees. Iora Health. Accessed on February 9, 2022. https://ioraprimarycare.com/boeing/
- 9 | Bleser W, et al Half a decade in, Medicare accountable care organizations are generating net savings: Part 1. Health Affairs Blog. September 20, 2018. https://www.healthaffairs.org/do/10.1377/forefront.20180918.957502/full/. Accessed November 8, 2022.
- 10 | Sullivan G, Feore J. Physician-led accountable care organizations outperform hospital-led counterparts. Avalere. October 15, 2019. https://avalere.com/press-releases/physician-led-accountable-care-organizations-outperform-hospital-led-counterparts. Accessed November 8, 2022.
- 11 | Business Group on Health. 2023 Large Employers’ Health Care Strategy and Plan Design Survey. https://www.businessgrouphealth.org/resources/2023-plan-design-health-care-delivery-system. Accessed November 8, 2022.
- 12 | Lapsey H. The Better Benefit Stack. 2018 Oliver Wyman Health Innovation Journal. https://health.oliverwyman.com/2019/03/the-better-benefit-stack.html
- 13 | Centers for Medicare & Medicaid Services. Medicare Shared Savings Program Continues to Grow and Deliver High-Quality, Person-Centered Care Through Accountable Care Organizations. CMS Newsroom. January 26, 2022. https://www.cms.gov/newsroom/press-releases/medicare-shared-savings-program-continues-grow-and-deliver-high-quality-person-centered-care-through. Accessed November 8, 2022.
- 14 | O’Reilly K. Doctor participation in ACOs, medical homes grows amid pandemic. American Medical Association. December 7, 2021. https://www.ama-assn.org/practice-management/payment-delivery-models/doctor-participation-acos-medical-homes-grows-amid. Accessed November 8, 2022.
- 15 | Avalere. MSSP Sees Continued Growth in Downside Risk ACOs. January 21, 2020. https://avalere.com/insights/mssp-sees-continued-growth-in-downside-risk-acos. Accessed November 8, 2022.
- 16 | Mechanic R et al. The 2018 Annual ACO Survey: Examining the Risk Contracting Landscape. Health Affairs Forefront. April 23, 2019. https://wwwhealthaffairs.org/do/10.1377/forefront.20190422.181228/full/. Accessed November 8, 2022.
- 17 | Business Group on Health. 2023 Large Employers’ Health Care Strategy and Plan Design Survey. https://www.businessgrouphealth.org/resources/2023-large-employers-health-care-strategy-and-plan-design-survey
- 18 | Business Group on Health. 2023 Large Employers’ Health Care Strategy and Plan Design Survey. https://www.businessgrouphealth.org/resources/2023-plan-design-health-care-delivery-system.
- 19 |Elkins K. Lowe's free surgery program helps cut costs, benefit employees. Charlotte Business Journal. March 30, 2016. https://www.bizjournals.com/charlotte/blog/outside_the_loop/2016/03/lowe-s-free-surgery-program-helps-slice-costs.html. Accessed November 8, 2022.
-
IntroductionValue-based Purchasing Employer Guide: Introduction

-
Executive SummaryValue-based Purchasing Employer Guide: Executive Summary
-
Part 1Definitions and Measures of Value in Value-based Purchasing
-
Part 2Value-based Reimbursement Strategies
-
Part 3Value-based Primary Care
-
Part 4Accountable Care Organizations and High-Performance Networks
-
Part 5Centers of Excellence
-
Part 6Value-based Virtual Care
-
Part 7Value-based Care Engagement Strategies
This content is for members only. Already a member?
Login
![]()